Hysteroscopy gives your fertility specialist a direct, high-definition view inside the uterus — something ultrasound alone cannot match. It identifies polyps, fibroids, adhesions, and septae that may be blocking implantation, and in many cases the problem is corrected during the same procedure. Thailand's accredited fertility clinics perform hysteroscopy routinely, with experienced gynaecologists and rapid scheduling, at a fraction of Western costs.
Hospital Stay
Day procedure (no overnight stay)
Request a Free Quote
Receive Your Plan
We Handle the Rest
Request a Free Quote
Receive Your Plan
We Handle the Rest
Free, no-obligation — you pay the hospital directly with no markup.
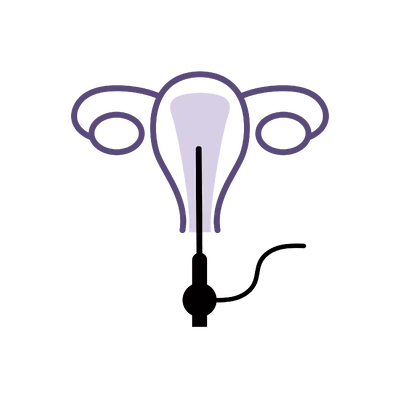
What Is Hysteroscopy?
Hysteroscopy passes a thin, lighted telescope through the cervix to examine the uterine cavity in real time. It is the gold standard for evaluating the uterus before fertility treatment — more accurate than ultrasound for detecting small polyps, thin adhesions, and subtle structural abnormalities that can prevent embryo implantation.
When pathology is found, operative instruments are passed through the hysteroscope to treat it in the same session — removing polyps, dividing adhesions, or correcting a uterine septum. This eliminates the need for a second procedure and means you can progress to IVF or embryo transfer sooner. For patients with recurrent implantation failure or unexplained infertility, hysteroscopy often reveals treatable findings that scans missed.
Common Concerns Hysteroscopy Can Address
- Recurrent implantation failure after IVF embryo transfer
- Abnormal uterine findings on ultrasound such as polyps or submucosal fibroids
- Unexplained infertility where standard investigations have not identified a cause
- Recurrent miscarriage with suspected uterine factor
- Abnormal uterine bleeding or irregular periods
Are You a Good Candidate?
- In good general health with no active pelvic infection
- Referred for hysteroscopy by a fertility specialist or gynaecologist
- Not currently pregnant
- Able to attend a pre-procedure consultation and the procedure within a 3–5 day window
Why Choose Thailand for Hysteroscopy?
Hysteroscopy is a short procedure, but accessing it quickly matters — especially when it is standing between you and your next IVF cycle. Thailand offers rapid scheduling and specialist care at a fraction of the cost.
Specialist
Experienced Gynaecologists
Our partner specialists perform diagnostic and operative hysteroscopy routinely as part of fertility workups, with high case volumes and modern equipment.
50–70%
Fraction of Western Costs
Hysteroscopy in Thailand costs significantly less than the same procedure in the US, UK, or Australia. You pay the clinic directly with no markup.
Days
Rapid Scheduling
No months-long waiting lists. Most patients move from consultation to procedure within a few days, keeping your fertility timeline on track.
Coordinated
Full Support Throughout
English-speaking clinical teams, a dedicated coordinator managing logistics, and clinics experienced with international fertility patients. Your care is well-organised from consultation through to follow-up.
Hysteroscopy Cost in Thailand
We do not charge for our service — you pay the clinic directly with no markup. Here is what hysteroscopy typically costs and how it compares internationally.
🇹🇭 Thailand
$1,200 – $2,640 (฿42,000–฿92,000)
🇺🇸 United States
$3,000 – $5,400
🇦🇺 Australia
A$2,600 – A$4,800
🇬🇧 United Kingdom
£2,400 – £4,200
Your Quote Will Include
- Specialist consultation
- Pre-procedure assessment
- Hysteroscopy procedure
- Sedation or anaesthesia
- Follow-up appointment
- Dedicated care coordinator
Prices are approximate and vary by technique, surgeon, and hospital. Your personalised quote will include a full cost breakdown.
Our service is free — you pay the hospital directly with no markup or hidden fees.
Get Your Free Quote
24hr Response
No Obligation
Care Coordinator
Average Cost of Hysteroscopy in Thailand
Hysteroscopy in Thailand typically costs between $1,200 and $2,200. A straightforward diagnostic hysteroscopy sits at the lower end. Operative hysteroscopy with polypectomy, myomectomy, or adhesiolysis costs more due to additional instruments, time, and pathology processing.
What Is Included?
Your quote covers the specialist consultation, pre-procedure assessment, the hysteroscopy procedure, sedation or anaesthesia, a follow-up appointment, and your care coordinator. Pathology fees for tissue analysis are discussed before the procedure if tissue removal is anticipated.
Cost by Hysteroscopy Type
Pricing varies by the complexity and scope of the procedure. Typical ranges at our partner hospitals in Thailand:
- Diagnostic hysteroscopy: $1,200–$1,500 — camera inspection of the uterine cavity, no surgical intervention
- Operative hysteroscopy (polypectomy or adhesiolysis): $1,500–$1,800 — removal of polyps, fibroids, or adhesions during the same procedure
- Hysteroscopy with endometrial biopsy: $1,700–$2,200 — combines visual inspection with tissue sampling for histology
Exact pricing is confirmed after your consultation and treatment plan are finalised.
Thailand vs International Price Comparison
Hysteroscopy in Thailand costs 50–70% less than the US ($3,000–$5,400), Australia (A$2,600–A$4,800), or UK (£2,400–£4,200). The savings reflect lower facility and specialist costs. Equipment and clinical standards are the same.
Types of Hysteroscopy in Thailand
Hysteroscopy can be purely diagnostic or operative — the difference depends on whether treatable pathology is found. Many procedures start as diagnostic and become operative when something is identified.
Diagnostic Hysteroscopy
A slender scope is passed through the cervix and sterile saline gently expands the uterus, providing a clear view of the endometrial lining, tubal openings, and cavity shape. The specialist inspects for polyps, fibroids, adhesions, and structural anomalies. Takes 10–15 minutes.
- Direct visualisation is more accurate than ultrasound for detecting uterine pathology
- Identifies subtle adhesions and small polyps that imaging may miss
- Often performed under light sedation for comfort
- Best for: pre-IVF assessment or investigation of unexplained infertility
Operative Hysteroscopy
When an abnormality is identified, operative instruments are passed through the hysteroscope to treat it in the same session. Common procedures include polypectomy, submucosal myomectomy, adhesiolysis, and septoplasty. This avoids a second anaesthetic and accelerates progression to fertility treatment.
- Polyps and small fibroids removed in minutes with minimal bleeding
- Adhesion division restores a normal cavity and may improve implantation rates
- Septum correction is associated with reduced miscarriage risk
- Best for: treating uterine pathology found on diagnostic hysteroscopy or prior imaging
Hysteroscopy Techniques Used in Thailand
Both diagnostic and operative hysteroscopy are performed through the natural cervical opening — no incisions, no scars. The technique used depends on what is found and what needs treating.
Diagnostic Visualisation
A high-definition camera on the hysteroscope projects a magnified image of the uterine cavity onto a monitor. The specialist systematically inspects the endometrium, tubal ostia, and cavity architecture. Sterile saline distension provides a clear field of view throughout.
- Real-time magnified view of the entire uterine cavity
- Systematic inspection of endometrium, tubal openings, and cavity shape
- Photographic and video documentation for your records
- Best for: thorough assessment of the uterine environment before fertility treatment
Operative Instruments
When pathology is identified, miniature graspers, scissors, or resectoscope loops are passed through the working channel of the hysteroscope. Polyps are excised, adhesions divided, and septa resected under direct vision. Modern bipolar energy systems reduce thermal spread and improve safety.
- Miniature instruments allow precise treatment under direct visualisation
- Bipolar energy systems minimise thermal injury to surrounding tissue
- Same-session treatment avoids the need for a second procedure
- Best for: removing polyps, dividing adhesions, or correcting uterine septae
Hysteroscopy Recovery Timeline
Day of Procedure
After a brief pre-procedure check, sedation or anaesthesia is administered and the hysteroscopy is performed. Most patients wake within minutes and rest at the clinic for one to two hours before being discharged. Mild cramping similar to period pain is typical and managed with over-the-counter painkillers.
Days 1–2
Most patients feel well enough to move around comfortably the following day. Light spotting or watery discharge may continue for a few days and resolves on its own. Avoid swimming, baths, and intercourse for approximately one week. Strenuous exercise should be avoided for a few days.
Day 3–5 — Follow-Up
A follow-up appointment reviews the hysteroscopy findings, discusses any pathology results if tissue was removed, and plans next steps for your fertility treatment. The optimal timing to proceed with IVF or embryo transfer is confirmed based on your recovery.
Returning Home
Most patients are comfortable to fly within two to three days of the procedure. You receive a detailed operative report and pathology results, which can be shared with your fertility team at home. Your care coordinator remains in contact to support your onward treatment plan.
Direct Visualisation
Gold-standard view of the uterine cavity
Diagnose & Treat
Problems corrected in the same session
Optimised for IVF
Uterine environment prepared for transfer
When Can You Fly After Hysteroscopy?
Most patients can fly one to two days after a diagnostic hysteroscopy. If operative work was performed — such as polyp removal or adhesion division — your specialist may recommend waiting two to three days to ensure initial healing is progressing well. A short follow-up before travel confirms you are ready to fly.
When Can You Resume Normal Activity?
Light activity can resume the same day or the following morning. Most patients feel back to normal within 24 hours of a diagnostic hysteroscopy. After operative hysteroscopy, avoid heavy exercise, swimming, and intercourse for approximately one week. Your specialist provides specific guidance based on what was done during the procedure.
When Will You Receive Results?
Visual findings from the hysteroscopy are available immediately — your specialist can tell you what was seen (and treated) as soon as the procedure is finished. If tissue was removed for pathology, laboratory results typically take three to five working days. Your care coordinator ensures these reach you and your home fertility team.
Risks and Safety of Hysteroscopy
Hysteroscopy is one of the safest gynaecological procedures, with serious complications occurring in fewer than 1% of cases. It is performed routinely at fertility clinics worldwide.
- Uterine perforation (very rare, fewer than 1 in 1,000 cases)
- Infection of the uterus or surrounding structures
- Bleeding — usually mild and self-limiting, occasionally requiring treatment
- Adverse reaction to sedation or anaesthesia
- Fluid overload from uterine distension media (rare, monitored throughout)
- Incomplete treatment requiring a follow-up procedure
Hysteroscopy is performed under continuous visual guidance — the specialist sees exactly what is happening at every moment. Accredited Thai fertility clinics follow international safety standards, including real-time fluid balance monitoring and modern bipolar energy systems that further reduce risk.
Is Hysteroscopy Safe in Thailand?
Yes. Our partner clinics operate within JCI-accredited hospitals or hold equivalent international accreditation. Specialists performing hysteroscopy have dedicated gynaecological training and high case volumes. Equipment, infection control, and safety monitoring protocols match the standards of any leading fertility centre.
How to Reduce Risks
Ensure the procedure is performed at an accredited facility by a specialist with specific hysteroscopy experience. Confirm that fluid balance monitoring is used throughout operative cases. Follow pre-procedure instructions regarding infection screening. If you have a known history of cervical stenosis or uterine surgery, inform your specialist in advance.
When Might a Follow-Up Procedure Be Needed?
If large fibroids or dense adhesions cannot be completely treated in a single session, a staged second hysteroscopy may be recommended. This is uncommon for standard polyp removal or septum correction. If intrauterine adhesions are divided, a follow-up hysteroscopy after one to two cycles may be performed to confirm the cavity remains open.
Top Fertility Clinics for Hysteroscopy in Thailand
The value of hysteroscopy depends entirely on the specialist performing it. Here is what to look for.
Accredited Fertility Clinics in Bangkok
Our partner clinics operate within JCI-accredited hospitals with dedicated fertility and gynaecological surgery units. They are equipped with the latest hysteroscopic equipment, including high-definition cameras, bipolar resectoscopes, and fluid management systems. These are established fertility centres, not general gynaecology practices.
Experienced Hysteroscopy Specialists
Our partner gynaecologists perform diagnostic and operative hysteroscopy as a core part of their fertility workup. They have specific training in intrauterine surgery and manage the full spectrum of uterine pathology — from small polyps to complex adhesiolysis and septum correction.
What to Look for in a Specialist
Confirm the specialist has dedicated experience in operative hysteroscopy, not just diagnostic. Ask about their experience with your specific finding — adhesions, polyps, or septae each require different skills. Check that the clinic uses modern bipolar energy systems and fluid monitoring. Ask whether same-session operative treatment is available so you do not need a separate procedure.
Before and After Results
Hysteroscopy results are measured in what is found, what is treated, and how it affects your next fertility step.
What Hysteroscopy Reveals
The procedure provides a definitive view of the uterine cavity — polyps, submucosal fibroids, adhesions, septae, and endometrial irregularities are identified with certainty. This is particularly valuable for patients with recurrent IVF failure, where a treatable uterine factor may have been missed on ultrasound.
Impact on Fertility Treatment
Removing endometrial polyps before IVF has been shown to improve implantation and pregnancy rates in multiple studies. Adhesion division restores a normal cavity for embryo implantation. Septum correction reduces miscarriage risk in subsequent pregnancies. For many patients, hysteroscopy is the step that changes the trajectory of their treatment.
Planning Your Trip to Thailand for Hysteroscopy
Three to five days covers everything comfortably. Here is how to plan it.
How Long to Stay in Thailand
Three to five days is sufficient. Day one covers the consultation and pre-procedure assessment. The hysteroscopy is performed on day two or three. A follow-up appointment reviews findings and plans next steps before you travel home. Many patients combine hysteroscopy with other fertility investigations during the same visit.
What Is Included
Your care coordinator schedules the consultation, procedure, and follow-up, and arranges transport to the clinic. The quote covers the specialist consultation, procedure, anaesthesia, and follow-up. Pathology fees are discussed before the procedure if tissue removal is expected.
Combining with Other Fertility Investigations
Hysteroscopy combines well with hormone testing, ovarian reserve assessment, semen analysis, or a full female fertility workup. If you are travelling to Thailand specifically for fertility investigation, bundling these procedures into a single trip maximises efficiency and minimises travel.
Common Questions About Hysteroscopy
Everything you need to know before your procedure
Three to five days is recommended. This allows time for consultation, the procedure, and a follow-up to review findings and plan next steps.
Most patients experience little or no pain during the procedure because it is performed under sedation or general anaesthesia. Afterwards, mild cramping similar to period pain is common and usually resolves within a day with over-the-counter painkillers.
Diagnostic hysteroscopy takes 10–15 minutes. Operative hysteroscopy may take 20–45 minutes depending on what needs treating. Total time at the clinic including preparation and recovery is around two to three hours.
After a straightforward diagnostic hysteroscopy, you may proceed to IVF in your next cycle. If polyps, fibroids, or adhesions were removed, waiting one to two menstrual cycles is usually recommended to allow the endometrium to heal.
There is strong evidence that treating uterine abnormalities before embryo transfer improves implantation and pregnancy rates. Removing polyps, submucosal fibroids, and adhesions before IVF can significantly increase the chance of a successful outcome.
No. Hysteroscopy is performed entirely through the cervix — there are no external incisions and no visible scars.
Most patients are comfortable to fly within two to three days of the procedure. Timing depends on your individual recovery and the complexity of any operative work performed.
The quoted price includes the specialist consultation, pre-procedure assessment, the hysteroscopy itself, sedation or anaesthesia, a follow-up appointment, and your care coordinator. Pathology fees for tissue analysis are discussed before the procedure.
Not everyone does. Hysteroscopy is recommended when there is a specific indication — abnormal ultrasound findings, recurrent implantation failure, or unexplained infertility. Some clinics recommend routine diagnostic hysteroscopy before a first IVF cycle as part of a thorough workup.
Hysteroscopy examines the inside of the uterus through the cervix. Laparoscopy examines the outside of the uterus, ovaries, and fallopian tubes through small abdominal incisions. They investigate different things and are sometimes performed together.
Nick Peplow
REVIEWED BY
Patient Care Director
Last reviewed: March 25, 2026